Weight Loss Surgery - Single Anastomosis Bypass
What is a Mini Gastric Bypass?
Mini Gastric Bypass Surgery (MGBP) is a relatively new procedure, which combines some of the properties of a Gastric Sleeve with a Gastric Bypass.
Mini Gastric Bypass Surgery is also referred to as Single Anastomosis Gastric Bypass (SAGB) surgery.
It is an operation that combines restriction with some malabsorption, and the result is that it provides good weight loss with great quality of life.
Do I Qualify for a Gastric Bypass?
You may be eligible for a gastric bypass if you have a body mass index (BMI) that is greater than 40 (or greater than 35 with weight-related illnesses) and you have tried all other types of diets without long-term success. In certain circumstances, patients with lower BMI may be candidates.
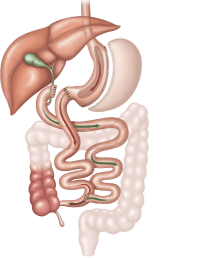
Single Anastomosis Gastric Bypass Procedure
The SAGB procedure is performed with a laparoscopic (keyhole) technique under general anaesthesia.
- The upper part of the stomach is divided into a tube, similar to the top three-quarters of a sleeve and then joined to a loop of intestine.
- Five small incisions (between 5 and 12mm in length) are made for the insertion of keyhole surgery instruments.
- Using these instruments, the top of the stomach is stapled to form a thin tube (30ml to 50ml in size). The thin tube becomes the new, smaller stomach and is completely separate to the rest of the stomach.
- This stomach is then sewn to a loop of the small intestine, bypassing the first part of the intestine called the duodenum and approximately 150-200cm of the bowel. The rest of the stomach and upper part of the small intestine remains in the body but is no longer used for food digestion.
How Does Single Anastomosis Gastric Bypass Work
The SAGB helps you to lose weight in two ways:
- Restricting the amount of food that can be eaten at any one time, thereby reducing meals to healthy portion size, and
- Decreasing the number of calories your body absorbs during digestion as food bypass about 200cm of your upper small intestine
Expected Weight Loss
Most people can expect to lose up 70% of their excess body weight over a 12 to 18 month period.
Advantages of a Gastric Bypass
- It is particularly effective for patients with a larger BMI as the procedure has more predictable weight loss outcomes.
- Most patients have an almost immediate reduction in their need for diabetic medication and some are able to completely stop diabetic medication altogether.
- It does not require any on-going adjustments which are required with other procedures, such as the gastric band. Regular follow up is however necessary to ensure weight loss is appropriate and intake is nutritionally adequate.
- It is effective for those people who tend towards high sugar or high-fat foods. Dumping syndrome is directly linked to a high-sugar, or high-fat intake. Symptoms of dumping are unpleasant and therefore discourage the intake of high-calorie sweet foods.
Disadvantages of a Gastric Bypass
Disadvantages of the SAGB bypass are generally related to the magnitude of the surgery:
- Complications, although rare, are generally more serious than with other weight loss procedures, such as the gastric band.
- There is a higher risk of nutritional deficiency due to the reduced absorption of vitamins and nutrients. Life-long vitamin and mineral supplementation is essential to prevent deficiency following surgery. Long term follow-ups with the surgeon and dietitian to monitor nutritional status is also very important.
Risks of a Gastric Bypass
As with any surgical procedure, the gastric bypass operation has risks which are important to clearly understand before proceeding.
The following is a comprehensive list of issues which can occur. The following is a comprehensive list of issues which can occur. Most of these complications are very rare and 90-95% of patients have no issues.
Possible Acute Complications
Acute complications include (but are not limited to):
- Bleeding - this occurs in less than 1 in 100 patients after the procedure. This may require blood transfusion or rarely reoperation.
- Infection – if an infection develops it may require treatment with antibiotics and can occasionally require reoperation.
- Leak - a leak of fluid can occur through the new join between the stomach and intestines if it does not heal well. This can happen in the first few days after surgery and may require reoperation. If these leaks persist they can leak to the skin or wound (known as a fistula) or cause a persistent fluid infection in the area (abscess). If this happens, length of hospital stay may be extended to weeks or even months after surgery, and it may be a life-threatening problem. This occurs in less than 1% of cases.
- Ulcers - Just like ulcers can occur in a normal stomach, they can also occur in the new stomach pouch after a gastric bypass. For this reason, patients need to take anti-ulcer medication for 6 months after surgery. Sometimes ulcers can still develop and require additional therapy to manage.
- Damage to Organs – any keyhole procedure can be complicated by unintentional injury to the organs near the area of operation. This may require a repeat operation to repair the damaged organs.
- Blood Clots – Deep Venous Thromboses (clots in the veins) and pulmonary embolus (clots in the lungs)
- Pneumonia/ Chest Infection
- We take measures directly aimed at reducing these risks, but if complications occur, additional treatment may be necessary.
Possible Long-Term Complications
- Wound Hernia – any wound of the abdominal wall has a chance, anytime in future, of developing a hernia (some of the bowel or fat from inside the abdomen can get stuck underneath the skin). If this happens it needs to be assessed, and if it is red, hot and painful it should be seen to quickly as it may be an emergency.
- Anastomotic Stricture – It is important to keep the new connection between the stomach and the intestines small so as to achieve the right amount of weight loss. Sometimes this means the connection is too tight (less than 1 in 10 patients). If this occurs it may require stretching under endoscopy (camera into the stomach).
- Internal Hernia – occasionally the loops of bowel in the abdomen can become entangled and get stuck. If this occurs, a re-operation is required to fix the problem. If there are any unexpected abdominal complaints it is important to be assessed quickly by the surgeon.
- Adhesions – any procedure in the abdomen can cause adhesions (scar tissue). This can occur any time after the operation and can sometimes cause problems with the bowel getting stuck or twisted. This may require hospitalization and may even require re-operation.
- Gastro-Oesophageal Reflux – If reflux occurs post-operatively some patients can require acid-suppressing medication. This operation should be avoided for those people with severe symptoms of reflux prior to surgery.
- Failure of weight loss/weight regain – this usually occurs when dietary advice is not followed. If you eat too much food at once this can stretch the small stomach pouch making it easier to take larger volumes at meal times in the future.
- Other - As this surgery affects the function of the gut, some patients are unable to tolerate adequate intakes of food which can result in the requirement of long-term nutritional support via intravenous methods, called TPN (total parenteral nutrition).
Dumping Syndrome
Dumping syndrome is a group of signs and symptoms that usually occurs due to poor food choices. It is the result of high sugar or high-fat foods passing too quickly into the small intestine. Symptoms can include cramping, nausea, dizziness, weakness and fatigue. More information about dietary advice to avoid dumping will be provided during your visit to the dietitian.
Pre-Operative Diet
When you have a date for surgery, you will be advised to follow a very low-calorie liquid meal replacement diet for 14 days prior to surgery. OptifastTM is the recommended meal replacement product and is available from your local Chemist. The diet helps you to lose weight, particularly from the liver and therefore optimizes the safety of the procedure. You will receive more detailed information about this when you see the dietician.
Post-Operative Care
Most people will stay in the hospital for three to five days after surgery. After the procedure, you will start on clear fluids only (water, black tea, broth, juices). These will need to be sipped slowly in small amounts. An x-ray study is performed after the operation to check the size of the stomach pouch and to exclude a leak from the new connection. You will then be able to have free fluids for the rest of your hospital stay. During the next 4 to 6 weeks, while your body heals, you will gradually increase the texture and volume of the food you take. Further information, including a dietary guidelines booklet, will be provided at your appointment with the dietician.
Surgeon
The first post-operative clinic visit will be arranged for about 1 to 3 weeks after surgery. At this appointment, your wounds will be assessed and any other issues will be discussed.
Dietitian
It is important to remember that surgery is an aid to weight loss. It is vital that eating behaviours are modified to get the best result from the procedure. It is important to eat a variety of healthy foods, to limit your intake of calorie-dense foods and liquids and to slow your speed of eating to improve food tolerance.
If eating behaviours are not adapted after surgery, weight loss will be limited or weight regain can be possible in the future. More detailed information about correct eating behaviours will be covered during your visit with the dietitian.
The dietitian will phone you within the first week following surgery to review your intake.
Your first post-operative clinic visit will be at 3 to 6 weeks following surgery and then 3 to 6 monthly thereafter.





